Last updated: May 2026
A palatal expander is a small orthodontic appliance that gradually widens the upper jaw. Most patients are children or teenagers, but adults can be candidates too. If your child’s orthodontist has recommended one, or if you’re an adult considering expansion treatment yourself, this guide covers what an expander actually does, what treatment looks like day to day, and what to ask your orthodontist before you start.
This is written by an orthodontic lab. We fabricate expanders for orthodontic practices around the country, which means we see the appliance side of treatment closely. Most of this article is for patients and parents. There’s a section near the end specifically for orthodontists evaluating expander options, clearly marked so you can skip it.
What a Palatal Expander Does
The upper jaw is made up of two halves connected by a seam called the mid-palatal suture. In children and younger teens, this seam hasn’t fully fused yet. A palatal expander applies steady outward pressure to the upper jaw, which gently separates the seam and lets new bone fill in the space. The result is a wider upper jaw that better fits the lower jaw and gives the teeth more room.
The appliance itself sits against the roof of the mouth and is anchored to the upper teeth or to small bone screws. A central screw is turned a tiny amount each day, usually by a parent at home. Each turn produces a small, controlled amount of expansion.
The reason expansion works well in children and teens is that the suture is still flexible. In adults, the suture has fused, which is why adult expansion typically requires a different appliance type or, in some cases, a small surgical procedure. More on this below.
Who Needs a Palatal Expander
Orthodontists recommend palatal expanders most commonly for these reasons:
Crossbite. When the upper teeth bite inside the lower teeth, instead of outside, the result is a crossbite. This happens because the upper jaw is narrower than it should be. Expansion fixes the underlying jaw width problem rather than just shifting the teeth, which means the correction tends to be more stable.
Crowding. When there isn’t enough room in the upper arch for all the permanent teeth to come in straight, expansion creates space. In some cases this can avoid the need for tooth extractions later in treatment.
Breathing and airway concerns. A narrow upper jaw often comes with a narrow nasal floor. Widening the upper jaw can improve nasal airflow and is sometimes part of the treatment plan for children who mouth breathe, snore, or have signs of sleep-disordered breathing. This is an area where orthodontics, pediatric dentistry, and sleep medicine increasingly overlap.
Impacted teeth. When a permanent tooth is stuck in the bone with no room to come in, expansion can sometimes create the space needed for it to erupt naturally.
The reason orthodontists tend to recommend expansion early, often between ages 7 and 12, is that the suture is most responsive during this window. Treatment is faster, more predictable, and doesn’t require the additional steps that adult expansion sometimes does.
For adults, expansion is still possible, but it usually involves a different appliance, most commonly MARPE or MSE. We cover those in the types section below, and we have a full practitioner guide to MARPE for adults if you’re an adult considering expansion.
What to Expect During Treatment
Here’s what treatment actually looks like, day by day.
The fitting appointment. The orthodontist seats the expander, usually in a single appointment. For tooth-borne expanders, bands are cemented around the back molars; for bone-anchored expanders, small screws are placed in the palate. The appointment itself isn’t painful. The first few days afterward, the appliance feels strange. Patients describe pressure, fullness, sometimes mild soreness when biting. This fades within about a week as the mouth adjusts.
The activation phase. This is the active expansion period. Each day (or every other day, depending on the prescription), a parent uses a small key to turn the expansion screw a quarter or half turn. Each turn produces a small amount of expansion, usually about 0.25mm. The activation phase typically lasts 3 to 6 weeks.
After each turn, there’s a feeling of pressure that lasts for a few minutes to a few hours. Children often describe it as their teeth feeling “tight.” This is normal and expected. The pressure is the appliance doing its job.
The gap. A few weeks into expansion, parents often panic when a visible gap appears between the two front teeth. This is not a problem. It’s evidence the expansion is working. The suture is separating, which is exactly what’s supposed to happen. The gap closes on its own once the expander stops actively widening, usually within a few months. The gap closing is not the orthodontist fixing a mistake. It’s the natural follow-through of treatment.
Eating. Food gets stuck in the expander. There’s no way around this. Soft foods are easier the first week. Hard, sticky, or chewy foods (caramel, taffy, hard candies, gum, ice) should be avoided for the entire treatment because they can damage or dislodge the appliance. Most patients adapt their eating habits within days.
Speech. Most patients lisp slightly the first few days. By the end of the first week, speech sounds normal again. Reading aloud at home for ten minutes a day in the first week speeds up the adjustment. Permanent speech effects are not a thing.
Hygiene. Brushing with the expander in place takes more time and more attention. A water flosser helps. The orthodontist will demonstrate the cleaning routine at the fitting appointment.
The retention phase. After active expansion ends, the appliance stays in place for several months while new bone fills in the expansion gap. The screw isn’t being turned during this time. The expander is just holding the new width steady so the bone can stabilize. This phase usually lasts 4 to 6 months.
Removal. When the orthodontist removes the appliance, the appointment is short and not painful. Some patients feel a brief pressure as the bands come off the molars. After removal, the next phase of orthodontic treatment, which is often braces or aligners, begins.
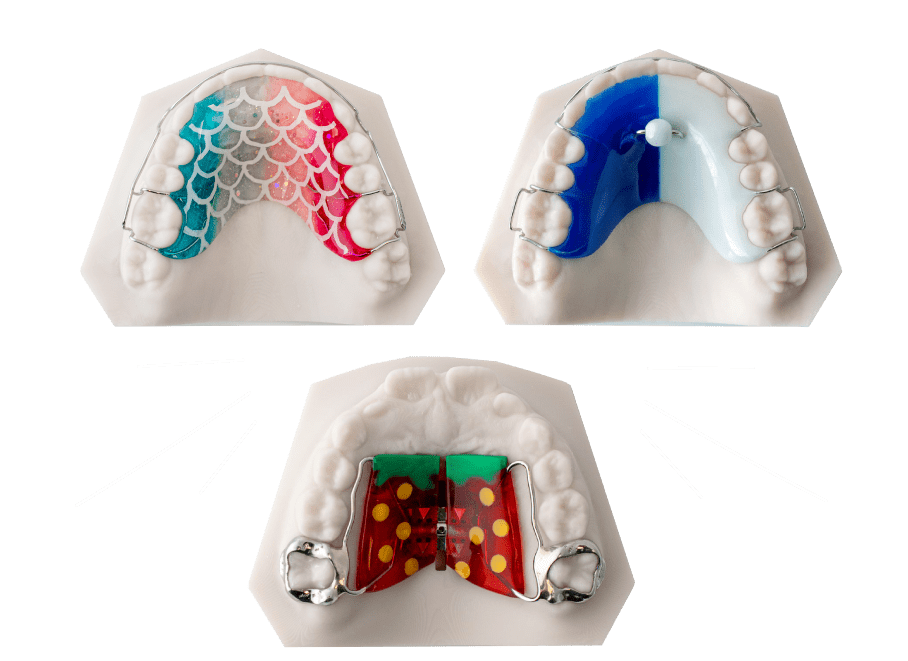
Types of Palatal Expanders
Different appliances suit different cases. The orthodontist chooses based on the patient’s age, the amount of expansion needed, the patient’s anatomy, and sometimes the patient’s compliance history (some appliances require more cooperation than others).
Hyrax / Rapid Palatal Expander (RPE). The most common expander for children and young teens. Tooth-borne, with bands cemented around the upper molars. Reliable, well-studied, and the default choice for most pediatric expansion cases. We have a more detailed page on RPE fabrication for orthodontists.
Haas expander. Similar to a Hyrax but with acrylic coverage along the palate. Some orthodontists prefer the Haas for cases where additional anchorage is needed or where the palate has unusual contours.
Quad helix. A slower expander, often used in mixed dentition (when baby and permanent teeth are both present). Activated by the orthodontist at appointments rather than by the parent at home. Useful when daily compliance would be a problem.
Removable expanders. Some mild cases can be treated with appliances the patient takes in and out. These rely heavily on patient compliance and aren’t appropriate for cases requiring significant expansion.
MARPE (Miniscrew-Assisted Rapid Palatal Expander). Bone-anchored expander used primarily in older teens and adults. Uses small implants in the palate to direct expansion forces into the bone rather than the teeth. The appliance of choice for adult cases where the suture is mature but not fully fused. See our practitioner guide to MARPE.
MSE (Maxillary Skeletal Expander). A bone-anchored expander similar to MARPE but with a different anchorage geometry. Often selected for adults over 30 with denser sutures. We cover the MARPE vs MSE comparison in detail.
SARPE (Surgically Assisted Rapid Palatal Expansion). When the suture is fully fused and bone-anchored expanders alone won’t work, a small surgical procedure separates the suture so an expander can then widen the jaw. This is the option for adults whose anatomy doesn’t allow non-surgical expansion.
The right appliance depends on the patient. The orthodontist’s CBCT (a 3D x-ray) is the most useful information for choosing between these options, particularly for adults.
How Long Treatment Takes
Two phases:
- Active expansion: 3 to 6 weeks of daily or every-other-day activation.
- Retention: 4 to 6 months with the appliance in place but no longer being activated.
Total expander time: usually 5 to 7 months.
After the expander comes out, the next phase of orthodontic treatment usually begins, often braces or aligners, depending on what the rest of the case needs. Total orthodontic treatment time including expansion is typically 18 to 30 months for children and longer for adult cases.
Common Concerns Parents Have
Will my child be in pain? Real soreness is rare. Pressure and tightness after each activation are common but short-lived. Over-the-counter pain relief, if the orthodontist approves it, handles the worst day or two. Most kids adapt quickly.
Will my child speak normally? Yes. The first week involves some lisping. Speech returns to normal within days as the tongue adjusts. Permanent speech effects don’t happen with properly fitted expanders.
That gap between the front teeth is alarming. It’s supposed to happen. It means treatment is working. The gap closes on its own after expansion ends.
Can the expander come loose? It can, occasionally. If a band loosens, food gets under the cement and the appliance can shift. Call the orthodontist if you notice the expander moving, hear clicking, or see a gap between the band and the tooth. Most loose bands are recemented in a single short appointment.
What if we lose the activation key? Call the orthodontist. They have spares. Skip the day’s activation if you have to wait. One missed day doesn’t ruin treatment.
My child won’t stop playing with it with their tongue. Normal. They’ll stop after the first week or two. Reminding them not to push or pull on it is reasonable; expecting them to stop entirely is not.
Signs to call the orthodontist: the expander moves or feels loose, your child can’t eat at all (not just preferring soft foods), severe pain that doesn’t fade within a few hours of activation, the activation key won’t turn, or any visible damage to the appliance.
For Orthodontists: What the Lab Needs
This section is for orthodontists evaluating ODL or evaluating expander fabrication generally. Patient readers can skip to the FAQ.
What the lab needs to fabricate a palatal expander that seats correctly the first time:
- A high-resolution intraoral scan. Digital, not analog. Lower-resolution scans force interpolation at the design stage, which shows up as fit issues at delivery.
- Clarity on expander type and screw specification. Hyrax, Haas, quad helix, MARPE, MSE; expansion screw capacity (8mm, 10mm, 12mm); activation rate; any band size preferences for tooth-borne designs.
- For bone-anchored designs (MARPE/MSE), CBCT review. Bone thickness at planned anchorage sites needs verification before fabrication, particularly for adult cases.
- Realistic turnaround expectations. Custom-fabricated expanders take days, not hours. Practices that build lab time into their treatment scheduling rarely have surprises.
ODL accepts digital scans through standard intraoral scanner workflows. Our 3D-printed RPE workflow shows what a fully digital expander fabrication path looks like end-to-end. For complex or non-standard cases, we walk through the case with the doctor before fabrication starts.
How a Palatal Expander Is Made
Most palatal expanders today are fabricated through a digital workflow: an intraoral scan from the orthodontist becomes a CAD model, the appliance is designed to match the patient’s specific palatal anatomy, and the framework is either bent and soldered (traditional) or 3D-printed and finished (digital). The expansion screw and any bands or anchorage components are integrated, and the appliance goes through a fit verification step before shipping.
The reason custom fabrication matters is that palates aren’t standard shapes. A prefab expander in three sizes can’t account for vault depth, rugae position, or asymmetry. A custom-fabricated appliance designed from the patient’s own scan fits correctly the first time, which means less chair time at the fitting appointment and fewer adjustments through treatment.
<a id=”faq”></a>
Frequently Asked Questions
Will it hurt?
Pressure after each activation is normal and lasts a few minutes to a few hours. Real pain is uncommon. The first day or two after the expander is fitted involves some general soreness as the mouth adjusts. Over-the-counter pain relief, with orthodontist approval, handles the worst of it.
How long does my child wear it?
About 5 to 7 months total. The first 3 to 6 weeks are the active expansion phase; the remaining 4 to 6 months are retention while bone fills in.
Will my child talk funny?
The first week involves a slight lisp. After that, speech returns to normal. Permanent speech effects don’t happen.
Will it leave a gap in their teeth?
A gap between the front teeth appears during expansion and is a sign treatment is working. It closes on its own within a few months after active expansion ends.
Is the expander permanent?
No. It’s removed after the retention phase. The new jaw width is what stays.
What if it breaks or comes loose?
Call the orthodontist. Most repairs are short appointments. Don’t try to push the appliance back into place yourself.
Can adults get expanders?
Yes, but the appliance type is different. Adult expansion typically uses MARPE or MSE rather than a tooth-borne RPE because the mid-palatal suture has fused. See our MARPE guide for the adult-focused version of this article.
Do palatal expanders help with breathing or sleep apnea?
For some patients, yes. Widening the upper jaw can increase nasal airway volume, which can improve nasal breathing and reduce mouth breathing in children. For adults with sleep-disordered breathing, expansion is sometimes part of a multidisciplinary treatment plan involving orthodontics, sleep medicine, and ENT. See our airway-focused expansion page.
How much does treatment cost?
Cost varies significantly by region, by orthodontist, and by case complexity. Insurance coverage varies too. Ask your orthodontist for a specific quote for your case.
What happens if we don’t do treatment?
That’s a conversation for your orthodontist. Untreated crossbite or significant crowding tend to get harder to address later in life, and adult expansion is more involved than pediatric expansion. The window where simple expansion works closes around the late teens.
A Last Note
Choosing the right expander for any patient is an orthodontist’s call, not an article’s. This guide covers the general landscape of palatal expansion treatment so you can have a more informed conversation with your provider, but the specific decision depends on a CBCT, a clinical exam, and your orthodontist’s judgment about what fits your case.
If you’re an orthodontist evaluating a lab for expander fabrication, submit a case for review and we’ll walk through the scan and Rx with you before fabrication starts. The AAO patient resource is also a useful general reference.