Last updated: May 2026
What a Tongue Crib Does (and When Orthodontists Prescribe One)
A tongue crib is a fixed orthodontic appliance for a specific kind of habit. Not every kid sucking their thumb needs one. Not every anterior open bite is a tongue thrust case. Knowing which habit you’re actually treating is most of the work, and choosing the appliance is the easy part once that’s clear.
This guide is for parents whose child has been told they need a tongue crib, and for orthodontists or pediatric dentists deciding which habit appliance fits a specific patient. ODL fabricates tongue cribs and the three other habit appliances in the same category, and most of what follows comes from the production-side view of when each one is the right call.
What a Tongue Crib Actually Does
A tongue crib is a fixed maxillary appliance with vertical metal fencing positioned behind the upper front teeth. The fencing creates a physical barrier that prevents the tongue from pushing forward against the incisors during swallowing or at rest. Stopping that forward tongue pressure is what allows an anterior open bite caused by tongue thrust to close on its own, and what prevents the upper incisors from flaring outward over time.
The appliance is bonded to molar bands and stays in the mouth for several months. It’s not removable. The fencing is what makes a tongue crib a tongue crib (other habit appliances use different mechanisms entirely, which is the next section). For the fabricated specs, see the vertical tongue crib product page.
When a Tongue Crib Is the Right Call
The vertical tongue crib has three main indications:
1. Anterior open bite caused by tongue thrust. The tongue pushes forward against the upper incisors during swallowing and at rest. Over time, this prevents the front teeth from closing properly and creates a visible gap between upper and lower incisors when the back teeth are together. The tongue crib blocks the forward pressure, and the open bite often closes on its own within a few months.
2. Anterior flaring secondary to tongue posture. Same mechanism, different result. Instead of an open bite, the upper incisors are tipping outward. The tongue crib stops the cause; orthodontic treatment can address what’s already happened.
3. Combined tongue thrust and thumb-sucking habit. When a patient has both habits, the vertical fencing addresses both at once. The fencing physically blocks the thumb from contacting the palate the same way it blocks the tongue.
The vertical tongue crib is most commonly prescribed for children in mixed dentition (typically ages 7 through 11), but indications extend to older kids and adolescents when the habit hasn’t broken on its own. Adult cases exist but are uncommon and usually involve airway-focused orthodontic treatment plans.
The appliance is not the right call when the open bite is severe enough to need aligner-based correction or surgical evaluation, when the patient has poor oral hygiene that would let plaque accumulate around the fencing, or when the habit is pure thumb-sucking without a tongue thrust component. The third case is where habit appliance selection most often goes sideways, which leads into the next section.
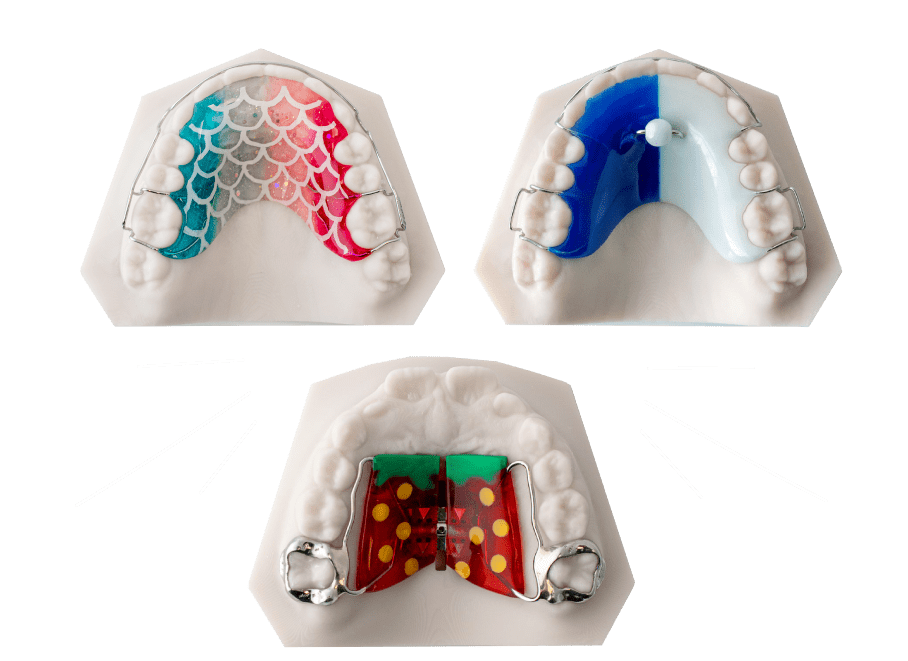
Tongue Crib vs the Other Habit Appliances
Four habit appliances cover most of what orthodontists prescribe in this category. They look similar from a parent’s perspective and overlap in some indications, but they’re not interchangeable.
Vertical tongue crib (fixed). Vertical fencing behind the upper anteriors. Best for tongue thrust, anterior open bite, and combined tongue + thumb habits. Fixed to molar bands.
Palatal crib, also called a thumb crib (fixed). A different kind of fence design positioned to block the thumb specifically. The geometry interferes with thumb placement against the palate without the tall vertical fencing of a tongue crib. Best for pure thumb-sucking with no tongue thrust component. See the palatal crib product page for the fabrication detail.
Rake appliance (fixed). Several small projections from a wire framework that physically interrupt the thumb or finger from settling against the palate. Functions similarly to a palatal crib but with a different mechanical approach. Sometimes preferred when a palatal crib has been tried and the patient has worked around it. See the rake appliance page.
Hawley with tongue crib (removable). A standard Hawley retainer with a tongue crib component built in. Removable, which means it depends entirely on patient compliance. Best when the patient can’t tolerate a fixed appliance or when the orthodontist wants the option to remove it for specific situations. See the Hawley with tongue crib page.
The most common Rx confusion ODL sees on habit appliances is which habit the appliance is being prescribed to address. A vertical tongue crib for a pure thumb-sucking case is overkill, adds plaque retention risk from the tall fencing, and doesn’t fit the indication better than a palatal crib or rake. The fabrication is what’s specified on the Rx, and the lab fabricates what’s ordered. For ambiguous cases (combined tongue thrust and thumb-sucking, or unclear etiology), the call before submission is worth the five minutes.
The decision frame is simpler than the appliance count makes it look:
- Pure tongue thrust or tongue-driven open bite, no thumb component → vertical tongue crib
- Pure thumb-sucking, no tongue thrust → palatal crib or rake
- Both habits present → vertical tongue crib (fencing addresses both)
- Patient won’t tolerate a fixed appliance → Hawley with tongue crib (compliance-dependent)
- Severe open bite or skeletal component → habit appliance alone won’t close it; talk to the orthodontist about a multi-stage plan
What Treatment Actually Looks Like
This section covers what to expect day by day, with the actual specifics rather than the hedged version.
The fitting appointment. The orthodontist seats the appliance in a single visit. Bands are cemented around the upper molars; the fencing is already in place on the framework. The appointment isn’t painful, but the first 24 to 48 hours afterward involve real adjustment. Patients describe pressure and a sensation of fullness against the tongue and palate. Soreness when biting is common. Both fade within a week.
Speech. The first few days, most patients lisp slightly. Speech returns to normal within a week as the tongue adjusts. Reading aloud at home for ten minutes a day in the first week speeds up the adjustment. Permanent speech effects don’t happen with a properly fitted tongue crib.
Eating. Food gets stuck in the fencing. There’s no way around this. Soft foods are easier the first week. Hard, sticky, or chewy foods (caramel, taffy, hard candies, gum, ice) should be avoided for the entire treatment because they can damage or dislodge the appliance. Most kids adapt their eating within days.
Hygiene. Brushing takes more time and more attention. Twice daily, three minutes per session, with a soft toothbrush. Plaque collects easily around the fencing and at the band margins, and inflammation is the most common reason a tongue crib gets removed early. A water flosser helps. The orthodontist will demonstrate the cleaning routine at the fitting appointment.
The habit breaking. The appliance does its job by being in the way. Patients can’t push their tongue forward against the incisors the way they did before, so the habit pattern that drove the open bite stops. Over weeks and months, the open bite closes on its own as the front teeth meet for the first time. Most tongue thrust habits resolve within four to six months of consistent appliance wear.
Removal. The orthodontist removes the appliance when the open bite has closed and the tongue habit has stopped. The appointment is short. Some patients feel brief pressure as the bands come off the molars. After removal, the next phase of orthodontic treatment (often braces or aligners, depending on the case) usually begins.
Things that should prompt a call to the orthodontist: the appliance feels loose or shifts, your child can’t eat at all (not just preferring soft foods), severe pain that doesn’t fade within a few hours of fitting or activation, a band or part of the fencing visibly damaged.
For Orthodontists: What the Lab Needs From Your Rx
This section is for orthodontists evaluating ODL or considering tongue crib fabrication generally. Parent readers can skip to the FAQ.
To fabricate a tongue crib that fits and functions correctly:
- Digital scan or PVS impression of the upper arch. Lower arch helpful but not required if the indication is tongue-only. STL or scanner export is fine.
- Bite registration. Without it, the lab can’t verify that the vertical fencing clears the lower anteriors when the patient closes.
- Band selection. AO Maximum Retention Bands, Leone Web Bands, or one of the AO slot variants depending on whether the case includes a fixed component. If not specified, ODL defaults to AO Maximum Retention Bands.
- Slot or headgear hook configuration if needed. Specify at Rx stage rather than asking for chairside additions later.
- Indication note. Tongue thrust, thumb habit, or both. This affects fence height and occasionally band selection.
- Occlusal rest preference. Recommended for almost all cases for stability against tongue and thumb forces. Default is yes unless noted otherwise.
For the fabrication detail and material specs, see the vertical tongue crib product page. To submit a case, use the standard ODL workflow.
When to Call Before You Submit
Some cases are worth a five-minute conversation before the Rx goes in:
- Combined tongue thrust and thumb-sucking when it’s unclear which is the primary driver
- Patient with significant arch asymmetry or non-standard palatal anatomy
- Compliance concerns where a removable Hawley with tongue crib might be the better starting point
- Cases where the orthodontist is debating between a tongue crib and a palatal crib for a borderline indication
Best case, the call confirms everything’s fine and the case ships standard. Worst case, the lab flags something now that would have been a chairside problem later. Either way, the conversation takes less time than a remake.
Frequently Asked Questions
Will a tongue crib hurt my child?
The first 24 to 48 hours involve real pressure and some general soreness as the mouth adjusts. After that, most kids report awareness of the appliance but no pain. Over-the-counter pain relief, with orthodontist approval, handles the worst day or two.
How long does a child wear a tongue crib?
Most cases run four to six months from fitting to removal. The appliance comes out once the open bite has closed and the tongue habit has stopped.
What’s the difference between a tongue crib and a palatal crib?
A tongue crib has tall vertical fencing behind the upper front teeth, designed to block the tongue. A palatal crib has a different fence geometry positioned to interrupt thumb placement against the palate. The tongue crib is for tongue thrust cases; the palatal crib is for pure thumb-sucking. Combined habits usually get a tongue crib because the fencing addresses both.
Can adults get a tongue crib?
Yes, but it’s uncommon. Most adult tongue thrust cases are addressed through orofacial myology therapy, sometimes alongside aligner-based bite correction. Adults considering a tongue crib should expect a full orthodontic workup that confirms the indication.
What if my child loses an attachment or breaks the appliance?
Call the orthodontist. Most loose bands are recemented in a single short appointment. Don’t try to push the appliance back into place yourself.
Will it affect my child’s speech?
The first week involves a slight lisp as the tongue adjusts to the fencing. After that, speech returns to normal. Permanent speech effects don’t happen with a properly fitted appliance. Reading aloud at home for ten minutes a day speeds up the adjustment.
Can my child eat normally with it?
Soft foods are easier the first week. After adjustment, most kids eat normally with two exceptions: hard, sticky, or chewy foods (caramel, taffy, hard candies, gum, ice) should be avoided for the entire treatment. Food getting stuck in the fencing is normal and is what the cleaning routine handles.
For more general patient information on habit appliances and tongue thrust, the AAO patient resource is a useful reference.
A Last Note
The tongue crib works when the indication is right. Choosing between the four habit appliances in this category isn’t about which one is best in the abstract; it’s about matching the appliance to the habit you’re actually treating. The orthodontist makes that call with a clinical exam. This article is meant to make the conversation between the orthodontist, the parent, and the patient easier to have.
If you’re an orthodontist considering ODL for a tongue crib or other habit appliance, you can submit a case for review and we’ll walk through the scan and Rx with you before fabrication starts.